Practice recommendations
- Only symptomatic hemorrhoids require treatment. Most patients can be treated with conservative therapy alone or an office procedure.
- Anoscopy detects more lesions in the anorectal region than does flexible sigmoidoscopy. Visualization is best achieved with the slotted anoscope.
- Rubber band ligation is the preferred office procedure for treatment of grade I/II hemorrhoids that do not respond to medical therapy, and treatment of all grade III hemorrhoids.
Most cases of hemorrhoids can be managed in the primary care setting with simple measures and office procedures, including anoscopy. This paper reviews the advantages, disadvantages, and levels of evidence regarding specific treatments for different grades of hemorrhoids.
Prevalence
Prevalence varies from 4.4% in the general population to 36.4% in general practice.1 The annual rate of office visits for hemorrhoids is 12 for every 1000 patients in the United States2 ; its prevalence is similar between the sexes and increases with age until the seventh decade.3,4 Only a third of patients with symptomatic hemorrhoids seek medical help.4
Characteristics
Hemorrhoidal padding, which is critical to maintaining continence, accounts for approximately 15% to 20% of the anal resting pressure and supplies important sensory information that enables the differentiation between liquid, solid, and gas. When an individual coughs or performs a Valsalva maneuver, this vascular padding increases in area and volume, thereby enabling the anal canal to remain closed and avoid the loss of stools.
Hemorrhoids are associated with chronic straining secondary to constipation, diarrhea, tenesmus, or long periods trying to defecate, and are common during pregnancy and child-birth.5 The pathophysiology is not clearly understood, but current theories suggest that structural or vascular changes may be involved.
The mucocutaneous junction of the ano-rectum, or dentate line, divides hemorrhoids anatomically into internal (above the junction) and external (below). This anatomic “border” is of special clinical interest because external pain fibers end at this point, and most people have no sensation above this line.
Hemorrhoids originating above the junction, even if prolapsed, are still classified as internal hemorrhoids, and are divided into 4 categories depending on the grade of prolapse:
- Grade I—Protrudes into the anal canal but does not prolapse
- Grade II—Prolapses but reduces spontaneously
- Grade III—Prolapses and requires manual reduction
- Grade IV—Irreducible prolapse.
Hemorrhoids, especially if external, sometimes thrombose (Figure 1). Distention of overlying perianal skin and inflammation associated with the process of thrombosis can cause severe pain and discomfort.
FIGURE 1
Thrombosed hemorrhoids Anoscopy
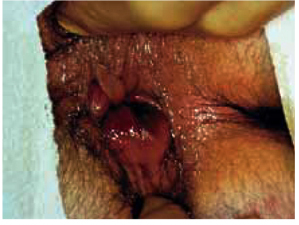
Thrombosis can be particularly painful due to distention of perianal skin and inflammation. Used with permission, National Procedures Institute, Midland, Mich.
Diagnosis
Symptoms
The most common symptoms of hemorrhoids are bleeding and prolapse. Less frequently, symptoms also include discomfort, pain, soiling, or itching.
Internal hemorrhoids are usually painless; bleeding or prolapse generally prompt a visit to the physician. Bleeding is described as bright red spotting on toilet tissue or as dripping in the toilet bowl and normally occurs at the end of defecation and separately from the stool.
External hemorrhoids may be asymptomatic, associated with discomfort, or a cause of acute pain in the event of a thrombosis. They generally do not bleed except in the case of a spontaneously resolved local thrombosis. Some individuals may have both types of hemorrhoids simultaneously (mixed).
The term hemorrhoids is commonly misused by patients to refer to any anal symptoms. Other diagnoses such as anal fissures, pruritus ani, abscess, fistula, and condyloma should be ruled out by examining the anus, the perianal region, and the anal canal. However, we have found no studies reporting on the accuracy of the medical history or the physical examination.
How to conduct a digital examination
The patient should be positioned in the left lateral decubitus position for the anorectal exam-ination.6 This position is more comfortable and less intimidating for the patient than the traditional head-down position, and it permits optimal visualization.
Digital palpation allows the entire circumference of the canal to be examined and rectal masses or tender points to be ruled out. Internal hem-orrhoids cannot be detected this way, however.6 The procedure, which must be done gently and with prior reassurance to the patient, is generally quite simple. Intense pain may prevent further examination and suggests the possibility of anal fissure or thrombosed external hemorrhoid.
Anoscopy: safe and essential office procedure
The most accurate method for examining the anal canal and distal rectum is anoscopy. Although several types of anoscopes are available, visualization is best achieved with the slotted anoscope (Figure 2).6 Once it has been inserted, the anoscope is gradually withdrawn while rotating right and left to allow inspection of the mucous membrane. Hemorrhoids appear as pink swellings of the mucosa. Ask the patient to strain during the examination to improve visualization.