Think you know how to fill out a death certificate? It’s often not as easy as it seems. Try the following cases.
Case 1
A 68-year-old woman is admitted to the ICU because of acute chest pain. She has a history of type 2 diabetes, hypertension, obesity, and angina. Over the next 24 hours an acute myocardial infarction is confirmed. Heart failure develops but improves with medical management. The patient then experiences a pulmonary embolus, confirmed by ventilation-perfusion lung scan and blood gases; over the next 2 hours she becomes unresponsive and dies.
Question: What should be written on the death certificate as the immediate and underlying cause of death? Answer: pulmonary embolus due to acute myocardial infarction due to atherosclerotic heart disease.
Question: What should be listed as conditions contributing to death but not directly causing death? Answer: type 2 diabetes, obesity, hypertension, and congestive heart failure.
Case 2
A 78-year-old woman has left hemiparesis from a stroke 2 years earlier. She has been unable to care for herself and has lived in a nursing home. She has had an indwelling urinary catheter for the past 6 months. Because of fever, increased leukocyte count, and pyuria, she is admitted to the hospital and started on 2 antibiotics. Two days later, the blood culture result is positive for Pseudomonas aeruginosa resistant to the antibiotics being administered. Despite a change of antibiotics, hypotension ensues and the patient dies on hospital day 4.
Question: What should be written on the death certificate as the immediate and underlying cause of death? Answer: P aeruginosa sepsis, due to a urinary tract infection due to an indwelling catheter, due to left hemiparesis, due to an old cerebral infarction.
Question: What should be listed as conditions that contributed to the death but that did not directly cause the death? Answer: nothing.
If you were correct on both cases, congratulations. If you were not, this article offers basic advice that will help you provide accurate medical information on death certificates.
Death certificates are important official records used for personal, legal, and public health purposes, yet they are frequently filled out inaccurately. Physicians are responsible for determining the cause and manner of death, yet they are seldom formally trained for this responsibility in medical school or residency. The result is frequent and avoidable errors.
Who is responsible for what?
Registration of deaths is a state responsibility. The National Center for Health Statistics compiles data from all states to produce national vital statistics, and most states use death certificate forms that conform to a recommended national standard. Though funeral directors are responsible for filing the certificate with the state, physicians are responsible for completing the medical portion of the certificate.
With the medical information provided, trained coders classify the cause of death using standardized methodology.
Medical examiners or coroners are responsible for investigating and certifying the cause of any death that is unexpected, unexplained, or resulting from injury, poisoning, or a public health threat.
Physicians are additionally responsible for answering inquiries from the registrar (these inquiries can be reduced by accurately and completely filling in the medical information) and submitting a supplemental report when autopsy findings or other information indicates a cause of death different from that originally reported.
How to complete the medical portion of the death certificate
The Figure is a standard certificate of death. It may vary slightly state to state. Physicians are responsible for items 24 through 49. If the state requires a pronouncing physician (Table 1), the pronouncing and certifying physicians may be different, in which case the pronouncing physician completes items 24 through 31 and the certifying physician items 32 through 49. If the pronouncing physician is also the certifying physician, items 26 through 28 need not be completed. If the death is referred to the coroner or medical examiner, they complete items 24, 25, 29, 30, and 32 through 49.
FIGURE
US standard death certificate
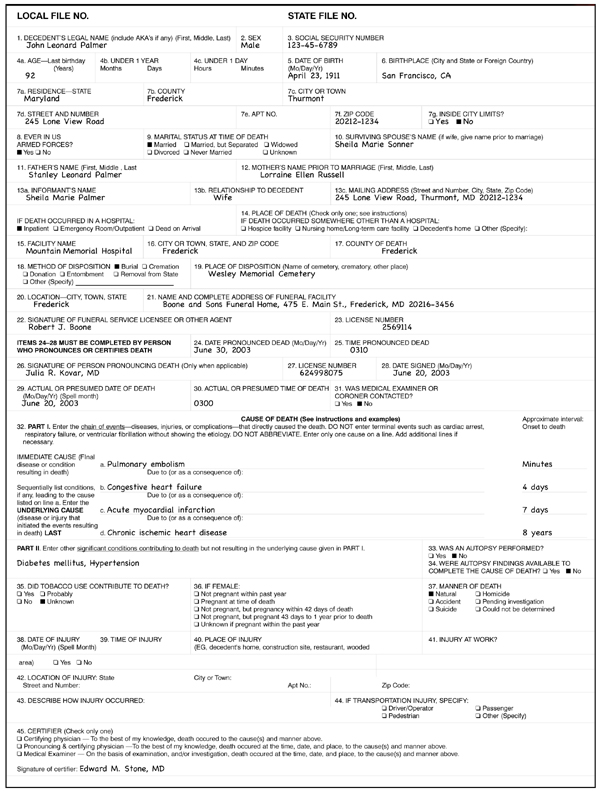
TABLE 1
Definitions
| Immediate cause of death:The final disease or injury causing the death. |
| Intermediate cause of death: A disease or condition that preceded and caused the immediate cause of death. |
| Underlying cause of death: A disease or condition present before, and leading to, the intermediate or immediate cause of death. It can be present for years before the death. |
| Manner of death: The circumstances leading to death—accident, homicide, suicide, unknown or undetermined, and natural causes. |
| Medical examiner: A physician, acting in an official capacity within a particular jurisdiction, charged with the investigation and examination of persons dying suddenly, unexpectedly, or violently, or whose death resulted from, or presents, a potential public health hazard. The medical examiner is not always required to be a specialist in death investigation or pathology. Most systems employing physicians as part time medical examiners encourage them to obtain training for medical examiners such as that offered by the National Association of Medical Examiners. |
| Coroner: A coroner is a public official, appointed or elected, in a particular geographic jurisdiction, whose official duty is to make inquiry into deaths in certain categories. In some jurisdictions, the coroner is a physician, but in many localities, the coroner is not required to be a physician nor be trained in medicine. |
| Pronouncing physician: The one who determines the decedent is legally dead. Not all states require a death to be pronounced by a physician. |
| Certifying physician: The one who certifies the cause of death. |