John D. Miller, BS Elizabeth Carter, BS Jonathan Shih, BS Nicholas A. Giovinco, DPM Andrew J.M. Boulton, MD Joseph L. Mills, MD David G. Armstrong, DPM, MD, PhD The Southern Arizona Limb Salvage Alliance (SALSA), University of Arizona College of Medicine, Tucson (Mr. Miller and Shih, Ms. Carter, and Drs. Giovinco, Mills, and Armstrong); Center for Endocrinology and Diabetes, Faculty of Health Sciences, University of Manchester, United Kingdom (Dr. Boulton) armstrong@usa.net
The authors reported no potential conflict of interest relevant to this article.
This brief exam will help you to quickly detect major risks and prompt you to refer patients to appropriate specialists.
› Screen for lower extremity complications at every visit for all patients with a suspected or confirmed diagnosis of diabetes. A › Consider implementing a risk-based referral system to connect primary screening with a specialist's care. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
Foot ulcers and other lower-limb complications secondary to diabetes are common, complex, costly, and associated with increased morbidity and mortality.1-6 Unfortunately, patients often have difficulty recognizing the heightened risk status that accompanies the diagnosis of diabetes, particularly the substantial risk for lower limb complications.7 In addition, loss of protective sensation (LOPS) can render patients unable to recognize damage to their lower extremities, thus creating a cycle of tissue damage and other foot complications. Strong evidence suggests that consistent provision of foot-care services and preventive care can reduce amputations among patients with diabetes.7-9 However, routine foot examination and rapid risk stratification is often difficult to incorporate into busy primary care settings. Data suggest that the diabetic foot is adequately evaluated only 12% to 20% of the time.10
In response to the need for more consistent foot exams, an American Diabetes Association (ADA) task force lead by 2 of the authors of this article (AB and DA) created the Comprehensive Foot Examination and Risk Assessment.5 This set the standard for the detailed investigation of lower limb pathology by a specialist, but was not well suited for other practice settings, including primary care. One reason is that it would be difficult to complete the comprehensive examination during a typical 15-minute primary care office visit. In addition, certain examination parameters require the use of neurologic and vascular assessment equipment and training not available in all health care settings.11
This exam takes substantially less time to complete than a comprehensive exam and eliminates common barriers to frequent assessment. With these thoughts in mind, we set out to develop an exam that could be done by a wide range of health care providers—one that takes substantially less time to complete than a comprehensive exam and eliminates common barriers to frequent assessment. The exam, which we’ll describe here, consists of 3 components: taking a patient history, performing a physical exam, and providing patient education. And best of all, it should only take 3 minutes.
The patient history (1 minute)
Patients may present with concerns about their feet, but may not be able to differentiate between benign and threatening symptoms. A thorough medical history can identify factors that may increase patients’ risk of developing lower-limb complications. Reviewing the patient’s medical history also can help guide the physical exam.
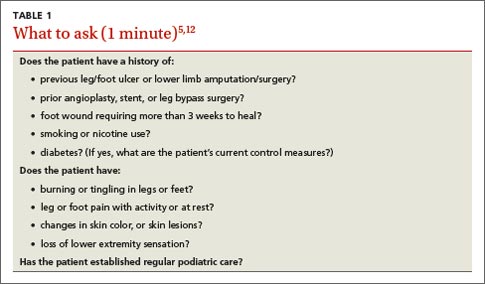
Review the patient’s diabetic history, blood glucose control, and previous diabetic complications. Ask patients about their history of peripheral vascular disease, quality of peripheral protective sensation, and previous lower-limb interventions and operations (TABLE 15,12). Patients with diabetes and suboptimal glycemic control have an increased risk for LOPS, chronic and recalcitrant ulcers, and wound infections.2 Additionally, patients with diabetes and a previous lower extremity amputation are at high risk for reulceration.5,12 Lastly, nicotine use and smoking are common pathogenic risk factors that contribute to peripheral artery disease (PAD).13
Physical examination (1 minute)
Careful inspection of the feet should be performed at every visit for patients with confirmed or suspected diabetes. Because up to 50% of patients with significant sensory loss due to neuropathy may be completely asymptomatic,14 failing to search for early signs of infection (FIGURE 1), skin breakdown, ulcer formation (FIGURE 2), skin temperature changes, and inadequate vascular perfusion may allow complications to develop.5 TABLE 25,15,16 outlines the essential components—dermatologic, neurologic, musculoskeletal, and vascular—of a rapid lower limb physical exam.
The dermatologic exam. This serves as a barometer for early intervention, and often results in a limb-saving referral to a specialist. Carefully examine the areas between the toes, where deeper lesions may go unnoticed. It should begin with a global inspection for discolorations, calluses, wounds, fissures, macerations, nail dystrophy, or paronychia.5 Skin discoloration or loss of hair growth may be the first signs of vascular insufficiency, while calluses and hypertrophic skin often are precursors to ulcers.5,17-19 Inspection of the toes should include a search for fungal, ingrown, or elongated nails. Carefully examine the areas between the toes, where deeper lesions may go unnoticed.5
The neurologic exam. Without protective sensation, patients with neuropathy are at a heightened risk of unrecognized injury and are unlikely to mention their deformities to medical staff.20-23 Consequently, skin deterioration may unknowingly progress to ulceration that requires extensive medical intervention or amputation.