William D. Anderson, III, MD, DABFM, FAAFP Nathaniel S. Treister, DMD, DMSc E.J. Mayeaux, Jr., MD, DABFM, FAAFP Romesh P. Nalliah, DMD University of South Carolina School of Medicine, Columbia (Drs. Anderson and Mayeaux); Brigham and Women’s Hospital, Boston (Dr. Treister); Harvard Medical School, Boston (Dr. Nalliah) william.anderson@uscmed.sc.edu
The authors reported no potential conflict of interest relevant to this article.
Being able to promptly recognize and diagnose oral lesions is critical to heading off several potentially serious conditions. This article and photo guide can help.
› Perform a biopsy and carefully monitor all potentially malignant oral lesions, including leukoplakia and erythroplakia. A › Consider evaluation for human immunodeficiency virus infection for any patient who has acute necrotizing ulcerative gingivitis/acute necrotizing ulcerative periodontitis, recurrent candidiasis, or oral hairy leukoplakia. A › Include melanoma in the differential diagnosis of oral pigmented lesions that have any features of cutaneous melanoma (eg, asymmetry, irregular borders, or variable or changing color). A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians can play an essential role in managing their patients’ oral health by promptly recognizing and diagnosing conditions that demand further medical attention, including non-odontogenic and odontogenic infections, primary oral mucosal diseases, oral manifestations of systemic disease, and malignancy. Many conditions are amenable to treatment by the family physician, while others will require referral to a specialist.
This article and accompanying photo guide describe the types of lesions you may encounter during examinations of the oral cavity, and the corresponding diagnoses.
Be vigilant for non-odontogenic conditions that may require urgent treatment
There are several uncommon, acute non-odontogenic conditions that affect the oral cavity that, when severe, can require urgent medical attention and possible hospitalization.
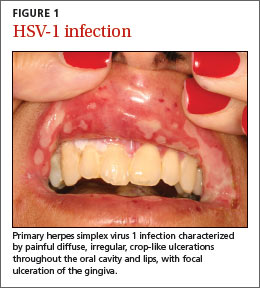
Primary herpes simplex virus 1 (HSV-1) infection is generally subclinical, but some patients develop significant oral disease—called primary herpetic gingivostomatitis—that’s characterized by painful diffuse, irregular, crop-like ulcerations throughout the oral cavity and lips1 (FIGURE 1). The gingiva is nearly universally affected, which distinguishes this condition from erythema multiforme and aphthous stomatitis, which are described below. The incidence is highest in children, followed by adolescents and young adults.2
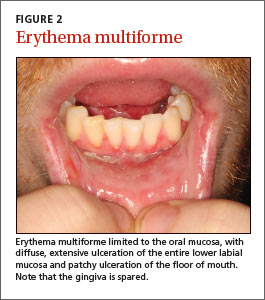
Erythema multiforme. This mucocutaneous hypersensitivity reaction can be limited to the oral cavity and lips, without accompanying skin lesions. Flu-like symptoms, including fever and chills, are followed by acute onset of diffuse oral ulcerations that are generally limited to non-keratinized mucosa, and spare the gingiva (FIGURE 2).3 Ulceration and crusting of the lips is common.
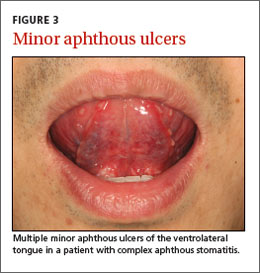
Aphthous stomatitis. Recurrent aphthous stomatitis (RAS) is a common immune-mediated inflammatory condition characterized by “canker sores,” or small round/ovoid ulcers with a well-defined erythematous halo (FIGURE 3). Lesions almost exclusively affect non-keratinized mucosa (and never the lip vermilion) and heal within 7 to 10 days, although “major” (>0.5 cm) lesions may persist much longer (FIGURE 4). A herpetiform pattern with multiple coalescing ulcers closely mimics HSV.
Small subsets of patients develop “complex” RAS, which is characterized by continuous and often multiple ulcerations that may extend into the esophagus, with associated chronic pain and compromised intake.2 RAS associated with systemic conditions is reviewed below.
How to spot signs of common dental diseases
In 2010 in the United States, close to 1.4 million emergency department visits and about $1 billion in hospital charges were due to dental problems.4 Approximately 40% of these visits were made by individuals without insurance.4 Due to a lack of dental insurance, patients may present to a medical professional rather than a dental professional. Additionally, uninsured individuals may neglect their dental problem until it becomes a medical emergency. Family physicians need to recognize dental disease and be able to provide basic management of emergencies.5
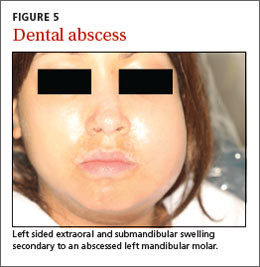
Dental abscess. A dental abscess can arise from pulpal infection (due to progression of caries) or periodontal infection (due to progression of periodontal disease). Pain symptoms are variable; however, intense, spontaneous cyclical pain is generally characteristic of a dental abscess of pulpal etiology, whereas a periodontal abscess can have less obvious symptoms. Swelling intraorally or extraorally indicates the spread of a localized infection (FIGURE 5).
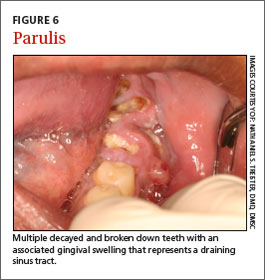
Severe infection and swelling can limit mouth opening and function, and in extreme cases may obstruct swallowing and even breathing (eg, Ludwig’s angina). Affected teeth may or may not demonstrate obvious findings of advanced dental disease, such as gross caries, fracture, heavy calculus deposits, or marked periodontal attachment loss. Oral examination may reveal a parulis (focal erythematous swelling of the adjacent gingiva with a central draining sinus tract) (FIGURE 6) and percussion of the affected tooth is generally painful.
Pericoronitis is infection and swelling of the gingival tissues that surround a tooth, typically in association with a partially erupted third molar. Signs and symptoms include pain, discomfort with eating and swallowing, and limited mouth opening. Examination demonstrates gingival inflammation around a tooth, with or without purulence (FIGURE 7).
Acute necrotizing ulcerative gingivitis (ANUG) and periodontitis (ANUP) are severe conditions that are typically associated with psychological stress, severe malnutrition, and immunosuppression in patients with preexisting gingivitis or periodontitis.6 ANUG is associated with intense gingival pain, halitosis, generalized erythema, and destruction of the gingival papilla, often with bleeding.7 ANUP is a more advanced condition associated with damage and loss of the periodontium (including bone), often with loose teeth (FIGURE 8).8