PRACTICE RECOMMENDATIONS
› Treat a simple cutaneous abscess from a methicillin-resistant Staphylococcus
aureus (MRSA) infection with incision and drainage alone. A
› Treat minor MRSA skin lesions in children with mupirocin. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A 21-year-old man seeks care at his family physician (FP)’s office for a painful, draining lesion that’s been on his left thigh for 5 days. He reports that he was bitten by a spider during one of his weekly football games with his fraternity brothers, but doesn’t recall seeing a spider. He has been applying an over-the-counter topical antibiotic without any improvement, and reports that the area of redness has tripled in size within the last 24 hours.
His past medical history is unremarkable except for an allergy to sulfa drugs that was discovered during treatment for a skin infection 2 years ago. He takes no regular medications.
The patient is afebrile and in no distress. The skin overlying his left thigh has a 1 cm oozing lesion with pus evident and surrounding erythema. The wound is warm and tender to the touch.
Based on the patient’s history, the FP suspects methicillin-resistant Staphylococcus aureus (MRSA) and obtains a swab for bacterial culture and sensitivities.
What the surveillance data tell us about MRSA
MRSA infections—a subset of staph infections that are resistant to beta-lactam antibiotics and cephalosporins—continue to be a major source of infection in the community.1 The prevalence of both community-acquired (CA) and hospital acquired (HA) MRSA infections worldwide has continued to grow despite improvements in controlling nosocomial spread.2,3 Data from the early 2000s found an approximate 1% to 2% MRSA colonization rate in the United States, but other countries have had rates as high as 50%.3 Rates across countries have consistently been higher in children and adolescents. A recent surveillance study suggests a decline in the incidence of the most serious types of MRSA infections in major metropolitan areas, the significance of which is still under investigation.4
CA-MRSA and HA-MRSA have different in vitro sensitivities to antimicrobials, different virulence factors, and different epidemiologic profiles.
CA-MRSA occurs in people who have not been recently hospitalized or had any recent medical procedures. These infections usually develop on skin and soft tissue. CA-MRSA typically contains the genes for the Panton-Valentine Leukocidin (PVL) toxin, which is a virulence factor that leads to increased interleukin-8 secretion and skin necrosis.5,6 In addition, CA-MRSA usually does not have genes associated with multidrug-resistant strains.
HA-MRSA occurs in people who have recently been hospitalized, had recent medical procedures, or have been treated in a longterm care setting. HA-MRSA is associated with multidrug-resistant strains; however, it usually does not have the genes for PVL toxin.7
Factors that put patients at risk for CA-MRSA skin infections
As many as 90% of CA-MRSA infections present as skin and soft tissue infections (SSTIs) that have the potential to become invasive if not managed appropriately.3,8 There are a number of factors that put patients at risk for these SSTIs (TABLE 1)7-9—chief among them, intrafamilial or close contact transmission. People living in close quarters with colonized individuals are 14 times more likely to be carriers than a matched unexposed population.9 Similarly, other environments that typically involve close quarters or overcrowding, including military installations, prisons, long-term care facilities, and daycare centers, generally see higher rates of MRSA colonization.10
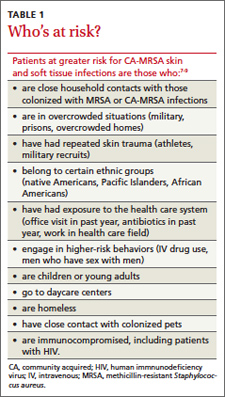
Researchers also hypothesize that repeated skin trauma is another risk factor for CA-MRSA SSTIs. This may explain the increased rates of CA-MRSA infections seen in athletes and military recruits undergoing basic training, as they are prone to skin abrasions.8 Certain ethnic groups have a higher prevalence of CA-MRSA infections as well, including Native Americans, Pacific Islanders, and African Americans.9,11 It is not entirely clear if there is anything unique predisposing these populations to MRSA or if this might be attributed to living in tight communities with close household contacts.
High-risk groups that have elevated rates of CA-MRSA SSTIs and are more likely to be carriers include intravenous drug users, men who have sex with men, immunocompromised individuals (including those with human immunodeficiency virus), and the homeless.8,9 Several studies have also reported higher rates of MRSA colonization and CA-MRSA infections in individuals who have come into contact with the health care system. A meta-analysis indicated that nasal swabs taken from patients at health care facilities were 2.35 times more likely to be positive for MRSA than those taken from individuals as nonhealth care locations.9 Risk factors such as antibiotic use or one or more physician visits in the past year have been associated with higher rates of infections, as well.2