Practice recommendations
- Injured limbs are traditionally rested by splint or cast. This is undertaken both for palliation and also in the belief that resting improves recovery time, and reduces complications such as deformity, functional problems and long-term pain.
- Early mobilization decreases pain, swelling and stiffness, particularly in the short term, without longer-term cosmetic or radiologic deformity. (SOR: A)
- Patients usually (but not always) prefer early mobilization, and return to work earlier. (SOR: C)
- Rest may be overused for limbs injury, although the extent to which early mobilization should be adopted needs more research. (SOR: C)
- The scope of limb injuries explored with trials of mobilization also needs further research.
ABSTRACT
Objectives: Rest is commonly used as primary treatment, rather than just palliation, for injured limbs. We searched the literature for evidence of benefit or harm from immobilization or mobilization of acute limb injury in adults.
Data Sources: We systematically searched for and retrieved randomized controlled trials (RCTs) of mobilization or rest for treatment of acute limb injuries, in Medline (1966–2002), EMBASE, Web of Science, and the Cochrane library, in all languages.
Review Methods: We examined patient-centered outcomes (pain, swelling, and cost), functional outcomes (range of motion, days lost from work) and complications of treatment.
Results: Forty-nine trials of immobilization for soft tissue injuries and fractures of both upper and lower limbs were identified (3366 patients). All studies reported either no difference between rest and early mobilization protocols, or found in favor of early mobilization. Reported benefits of mobilization included earlier return to work; decreased pain, swelling, and stiffness; and a greater preserved range of joint motion. Early mobilization caused no increased complications, deformity or residual symptoms.
Conclusions: We should not assume any benefit for immobilization after acute upper or lower limb injuries in adults. Rest appears to be overused as a treatment. More trials are needed to identify optimal programs for early mobilization.
We know that bed rest generally is over-prescribed.1 But what about resting or immobilizing acutely injured limbs—from simple sprains to gunshot wounds? This specific application of rest is controversial.2-6
Theoretically, rest should reduce further tissue damage by limiting movement, decreasing pain and swelling, and lessening loss of fracture reduction.7-15 However, mobilization increases blood flow and so reduces muscle atrophy, disuse osteoporosis, adhesions, and joint stiffness.7-15
The first empirical trials to determine whether rest or mobilization would offer greater benefit were undertaken in the 1980s, using both human and animal models. Systematic reviews have looked at specific injuries: acute ankle sprains16; ankle ligament rupture17; isolated ulnar fracture18; metacarpal fractures19; collateral ankle ligament sprains20; and soft-tissue ankle injury.21 Each review independently suggests benefits for early mobilization.
However, most clinicians employ some period of enforced rest of injured limbs. For example, a survey of orthopedic surgeons in Denmark found early mobilization for ankle fractures is prescribed for only 6% of patients.22
We systematically reviewed the literature to find trials that compared rest with early mobilization in acute limb injuries.
Methods
Protocol and search strategy
We searched the literature to identify prospective randomized controlled trials (RCTs) comparing rest with mobilization for acute limb injuries, searching the Cochrane Controlled Trials Register and Systematic Reviews, Medline (1966–2002), EMBASE (Rehabilitation and Physical Therapy), and Web of Science, combined with the following terms:
- immobilis*, immobiliz*, mobilis*, mobiliz*,
injur*, fracture*, limb*, cast*, brace*, splint*,
leg*, arm*, wrist*, elbow*, joint*, *carpal*,
*tarsal*, knee*, ankle*, femur*, tibia*, fibula*,
colles*, ulna*, radi*, humer*, sprain*, soft tissue,
plaster slab, dislocat*
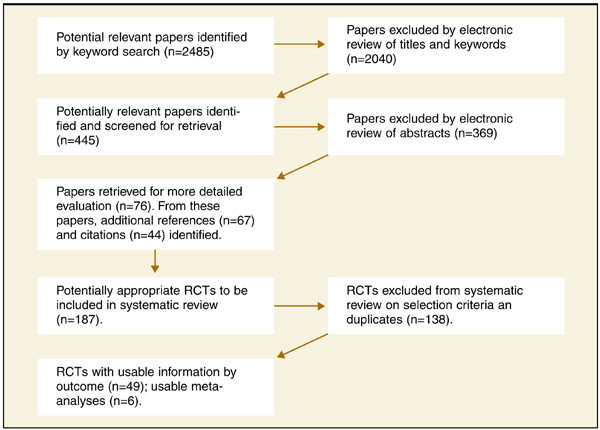
We accepted all publication languages and translated several papers. We found 445 potentially relevant papers by examining their titles or abstracts (Figure). Studies that did not fulfill our inclusion criteria were discarded.
We obtained full texts for 76 studies and undertook a prospective cited reference search in Web of Science for each study to identify more recent articles. A total of 187 papers were then evaluated further for duplicate data and inclusion criteria.
Trials that met our inclusion criteria:
- Were randomized and controlled
- Studied acute limb injuries
- Compared groups whose only treatment difference was mobilization (studies that compared surgery and immobilization against nonsurgical early mobilization were not included; studies with internal fixation were included only if internal fixation was applied to both groups)
- Had loss to follow-up of 20%, except where analysis was clearly intention to treat
- Studied populations not focussed solely on young children, (studies in which the given age range included a small number of patients as young as 11 or 12 years were accepted—in these studies the median age was much higher)
- adequately reported data collection and statistical analysis.
By these criteria, we excluded 138 studies (a list of which is available from the authors). Finally, 49 studies were included.
FIGURE
Literature search process, and methods by which randomized controlled trials (RCTs) were selected